
Careful evaluation and description of heart murmur characteristics can yield a good list of differential diagnoses, including types of heart disease that may be associated, and in some cases even a presumptive diagnosis. This is based primarily on a combination of the timing and the point of maximal intensity (PMI) of the heart murmur.
Other features of the murmur also aid in identifying the etiology and they include:
- The intensity (loudness)
- The frequency (pitch)
- The configuration (shape)
- The quality
- The duration
- The direction of radiation
These other features are of secondary use compared to the primary features of timing and PMI.
Point of Maximal Intensity (PMI)
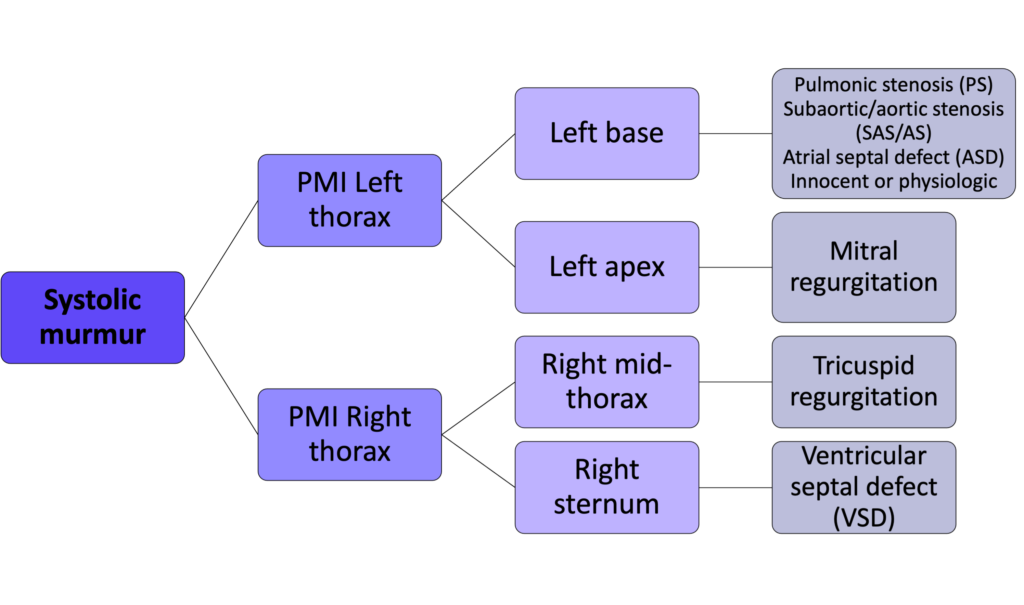
The point of maximal intensity (PMI) refers to the location where the murmur is loudest. The left chest wall is typically divided with respect to PMI into two focal areas:
- left heart base – includes both the pulmonary valve and aortic valve areas, as discriminating between these two is often not possible in small animals
- left heart apex – mitral valve area
The right chest wall is typically divided with respect to PMI into two focal areas:
- mid heart – tricuspid valve area
- sternal border – VSDs in small animals may be heard loudest here
Timing
Timing of heart murmurs is generally divided into one of three classes:
- systolic (occurring during systole, between S1 and S2)
- diastolic (occurring during diastole, after S2 and before the following S1)
- continuous (present at all times)
Systolic murmurs:
- Systolic murmurs represent the most common timing for murmurs identified in small animals
- When soft they are usually early in systole and disturb the end of S1. S1 often sounds slurred in these cases as opposed to ending abruptly as is normally the case.
- The careful clinician focuses on the end of S1 for soft systolic murmurs
- Holosystolic murmur: refers to a systolic murmur that begins during or immediately after S1 and ends with the onset of S2
- Pansystolic murmur: refers to a systolic murmur that begins during or immediately after S1 and continues into and obscures S2 (left ventricular pressure continues to be greater than left atrial pressure after aortic valve closure – during isovolumetric relaxation – thus mitral regurgitation can continue)
Systolic Murmur Examples:
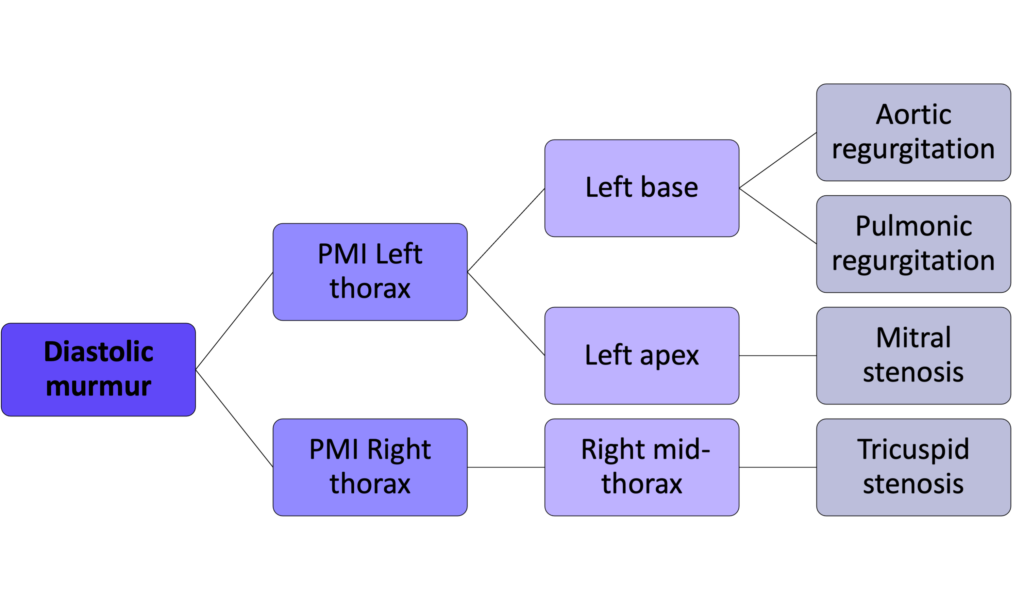
Diastolic murmurs:
- Very rare in small animals, especially in isolation
- More common in large animals, particularly in horses with aortic valvular insufficiency
- Often low frequency when present in small animals and often low intensity
- Better heard with the bell of the stethoscope in some cases if low frequency
Continuous murmurs:
- Second most common (to systolic) in small animals
- Most commonly associated with a patent ductus arteriosus (PDA), but may also be associated with arteriovenous fistulas or other systemic to pulmonary vascular connections
- Usually vary in intensity throughout the cardiac cycle (louder in systole, quieter in diastole), however the murmur is detected at all times
- The continuous nature of the murmur may only be noted at the PMI, while at other locations it may only be systolic, for example.
Continuous Murmur Examples:
To and Fro murmurs:
- The term for murmurs with both a systolic component and a diastolic component due to different etiologies that coexist.
- Examples include pulmonary stenosis with pulmonary insufficiency, aortic stenosis with aortic insufficiency, and ventricular septal defect (VSD) with aortic insufficiency.
- These murmurs differ from continuous murmurs in that the diastolic component does not last throughout diastole (often only in early diastole) and therefore it is not truly continuous.
To and fro Murmur Example:
Using the timing and PMI of a murmur, the following algorithms may be used to arrive at differential diagnoses:
Recall causes for a continuous murmur: PDA or arteriovenous fistula
Intensity:
The intensity of the murmur at its origin is related to (Blood flow velocity) x (Rate of flow). Overall, the intensity of a heart murmur is not related to the severity of the lesion or underlying disease; however, for some specific diseases there is a rough correlation between the intensity of the murmur and the severity of the lesion such as outflow stenoses.
The intensity of a murmur is graded on a scale of 1 to 6:
- Grade 1 – a very soft, focal murmur detected only with extended listening under quiet conditions
- Grade 2 – a soft murmur, heard within a few seconds but localized to a small area
- Grade 3 – a moderately intense murmur that is easily detected
- Grade 4 – a moderately intense to loud murmur that is easily detected
- Grade 5 – a loud murmur accompanied by a precordial thrill (palpable vibration) over the point of maximal intensity
- Grade 6 – a very loud murmur accompanied by a precordial thrill and the murmur is still heard when the stethoscope is pulled slightly off the chest wall
Heart Murmurs in Cats
- In the cat, the areas of typical localization for murmurs in dogs are not as useful. Murmurs in cats may be localized to the cranial or caudal thorax, and are often loudest along the sternum or just to the left or right of the sternum.
- Functional murmurs are relatively common in cats and frequently localized to the cranial sternum, associated with dynamic outflow tract obstruction.