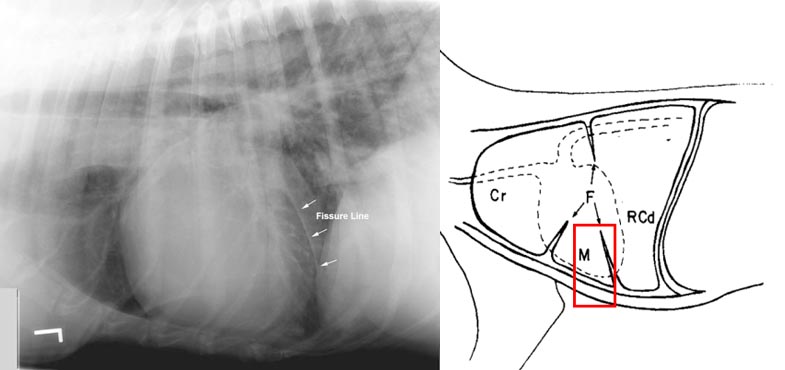
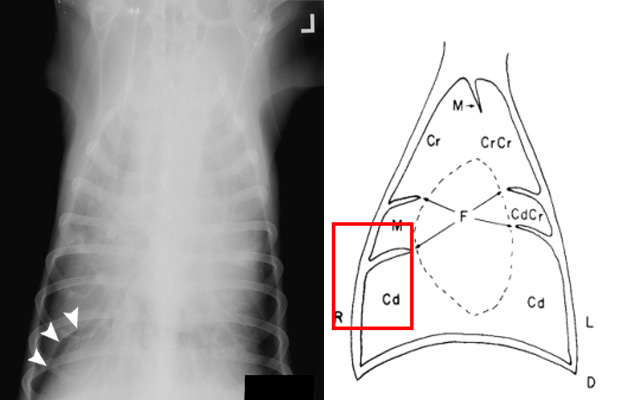
Pleural Fissures are the normal divides between the lobes of the lungs; they are not normally visible radiographically, but become radiographically visible in the presence of fluid in the pleural space or under conditions that cause the pleural lining of the lung to become thickened. It should be noted that the most common cause of fissure lines is pleural thickening. When there is pleural effusion however, the fluid collects within the fissure, wedges the lobes apart (with an agent [fluid] that contrasts with the radiopaque lungs) making the fissure radiographically visible. The fissure will generally appear as a discrete radiopaque line. Fissure lines created by pleural fluid are wider at the lung lobe margins and become narrower centrally. If a linear structure is observed in an area that doesn’t normally have a lung fissure, then other differentials must be investigated.
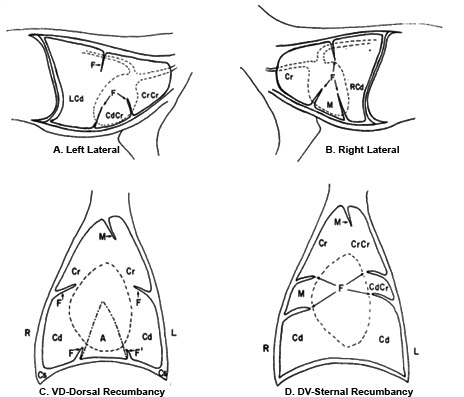
A – Fissures of the lateral aspect of the left lung (looking medial to lateral), usually seen when patient is in left lateral recumbency.
B – Fissures located on the lateral aspect of the right lung (looking medial to lateral), usually seen when patient is in right lateral recumbency
C – Fissures located on the dorsal aspect of the lungs and are seen when the patient is in dorsal recumbency.
D – Fissures located on the ventral aspect of the lungs and are seen when the patient is in sternal recumbency.